Play5min 00secAnnandale watches special session for broadband helpMay 28, 2015 7:44 AMBy Dave PetersAnnandale managed to get an earmark for broadband funding in legislation this year, but Gov. Mark Dayton vetoed the bill, asking for more money for rural broadband but objecting to the city's special treatment.
DNR pushes ahead with its groundwater planningFebruary 4, 2015 7:44 AMBy Dave PetersThe DNR's new approach makes it clear the agency retains ultimate authority over groundwater pumping but promises that stakeholders will get all the information they need.
Broadband providers seek $44 million from state fundNovember 12, 2014 5:04 AMBy Dave PetersAll the money must go to projects that will provide high-speed Internet access to areas that have no or poor service.
Shifting rain could be lowering groundwaterOctober 28, 2014 6:14 AMBy Dave PetersNew satellite data shows a decline in Minnesota's groundwater supplies and one scientist suggests a reason in addition to irrigation pumping might be that rain is falling at different times.
Satellite: A better way to measure groundwater levels?September 18, 2014 6:00 AMBy Elizabeth DunbarResearchers are using satellite data to measure groundwater use and how much is left. A key scientist will talk about the effort tonight in St. Paul.
Dayton panel seeks $200 million more for broadbandSeptember 4, 2014 7:59 AMBy Dave PetersThe state's task force advising Gov. Mark Dayton on high speed Internet access has told the administration it should seek another $200 million in next year's legislative session.
Judge won’t place blame for White Bear Lake water woesSeptember 3, 2014 8:59 AMBy Elizabeth DunbarRamsey District Judge Margaret Marrinan refused to decide by summary judgment whether the Minnesota Department of Natural Resources is at fault for the low water levels in White Bear Lake.
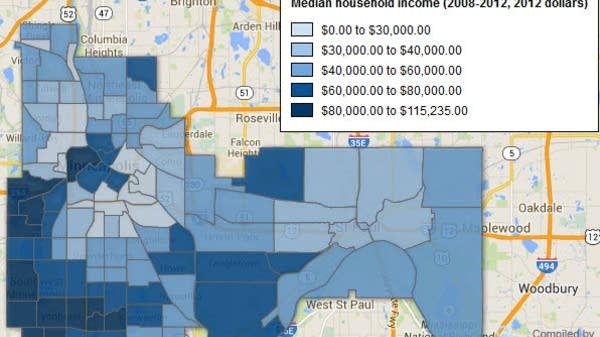
Who’s my neighbor? New Twin Cities maps tell the storyAugust 15, 2014 5:07 AMBy Dave PetersWilder Research in St. Paul has revamped its demographic profiles of Minneapolis and St. Paul neighborhoods, making the information much easier to use.
U of M flushes toilets with rainwaterAugust 5, 2014 6:00 AMBy Elizabeth DunbarNew student housing at the University of Minnesota includes a system for collecting stormwater from the roof and using it to flush the toilets for 600 students.
$50M pipe might not restore White Bear Lake levelsJuly 23, 2014 11:54 AMBy Elizabeth DunbarA draft of a report by the Metropolitan Council says shifting some suburbs' reliance from groundwater to Mississippi River water could cost hundreds of millions of dollars. It also says piping water from the river to raise levels in White Bear Lake would cost $50 million but leave officials uncertain of the impact.